


Case Study – Everything is Backwards (CCTGA)
Imaging Findings
Both CT and MR demonstrate atrioventricular discordance and ventriculoarterial discordance diagnostic of CCTGA. Both images also demonstrate situs inversus totalis. In addition, MR offered the benefit of evaluating the severity of the VSD shunt using phase contrast MR imaging with Q-flow analysis taken above the pulmonary and aortic valves. The Vp/Vq ratio measured 2:1. The severities of the valve abnormalities were also better evaluated using MR, which demonstrated moderate tricuspid insufficiency, mild aortic and pulmonic valve insufficiency, moderate subpulmonic, and mild pulmonary valve stenosis. The left atrium was mildly dilated at 5 cm and the systemic ventricle was minimally dilated with a systemic ventricular end-diastolic diameter of 5.8 cm. The systemic ventricular ejection fraction (morphologic right ventricle) was also slightly decreased measuring 40%.
Discussion
Congenitally corrected transposition of the great arteries (ccTGA) is a rare form of congenital heart disease occurring in less than 1% of congenital heart disease approximately 1/33,000 live births (1,2). It is characterized by atrioventricular and ventriculoarterial discordance and is associated with a variety of intracardiac defects. Most patients with ccTGA will have 1 or more associated cardiac anomalies. Common associated cardiac anomalies include VSD 60-80%, pulmonary stenosis involving the subpulmonic and/or valve level in ~ 30-50%. Some abnormality of the systemic AV valve occurs in up to 90% of patients (3). When patients are older, heart failure and cardiac arrhythmias can appear. This is caused by progressive failure of the morphological right systemic ventricle that is under high systemic pressures and often results in tricuspid valve insufficiency as this valve and morphological right ventricle are not as efficient in handling the increased pressure of the systemic circulation. Congenital corrected TGA (ccTGA) is usually associated with normal situs (situs solitus) however, it can be associated with situs inversus in ~ 5% of patients with CCTGA.
The systemic AV valve and systemic RV function are the most prognostic factors determining survival in patients with ccTGA and according to the study of Prieto4, there was aassociation with systemic AV valve regurgitation (SAVVR) with systemic RV dysfunction suggesting a causal relationship. In this study, they found that 65% percent of patients with SAVVR also had systemic RV dysfunction while 96% of patients without SAVVR had preserved normal RV function. Also of note in this study is the rapid rate of deterioration of the systemic RV once SAVVR was demonstrated. They found that the mean time from onset of SAVVR to systemic RV failure was only 5 years suggesting that SAVVR appears to be central to the progression to systemic RV failure and early death in patients with ccTGA. RV dysfunction may not be reversible if valve repair or replacement is delayed (5). The weakened systemic RV also compromises surgical outcomes and it is suggested that frequent surveillance of the systemic AV valve in patients with ccTGA and early intervention when SAVVR is recognized may help prevent the progression of SAVVR leading to systemic RV dysfunction (5).
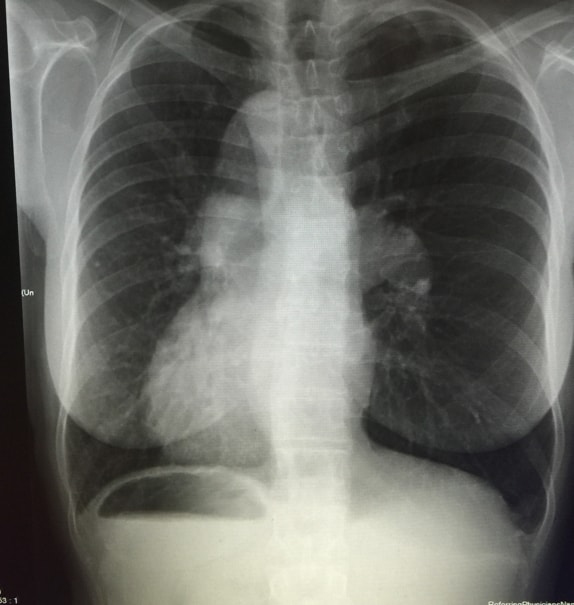
While chest x-ray, and echocardiography should be the initial imaging work-up of patients with complex congenital heart disease, CT and MRI are often useful in further elucidating the complexity of these disorders. MRI offers some advantages over CT in that there is no ionizing radiation and physiologic information can be obtained using phase contrast imaging and Q-flow analysis to obtain a more reliable estimate of the severity of potential shunts or cardiac valve abnormalities.
Bibliography:
-
Connelly MS, Liu PP, Williams WG, Webb GD, Robertson P, McLaughlin PR. Congenitally corrected transposition of the great arteries in the adult: functional status and complications. J Am Coll Cardiol. 1996;27:1238–1243.
-
Carole A: Warnes. Transposition of the Great Arteries.
Circulation 2006, 114:2699-2709. -
Allwork SP, Bentall HH, Becker AE, et al. Congenitally corrected transposition of the great arteries: morphologic study of 32 cases. Am J Cardiol. 1976;38:910–923.
-
Prieto LR, Hordof AJ, Secic M, Rosenbaum MS, Gersony WM. Progressive tricuspid valve disease in patients with congenitally corrected transposition of the great arteries. Circulation. 1998;98:997–1005.
-
Van Son JA, Danielson GK, Huhta JC, et al. Late results of systemic atrioventricular valve replacement in corrected transposition. J Thorac Cardiovasc Surg. 1995;109:642–652.
Authors’ information
-
Joshua Ian Gottlieb; NYIT College of Osteopathic Medicine; Northern Boulevard; Old Westbury, NY, 11568; joshgottlieb@sbcglobal.net.
-
Roy Gottlieb, D.O., FSCCT; Medical Director, Rolling Oaks Radiology; 415 Rolling Oaks Drive, Suite 125, Thousand Oaks, CA 91361; (818) 398-4928 cell; (805) 778-1513 work; roygottlieb@sbcglobal.net ; corresponding author.



Add new comment